Coronavius may be easier than the flu, but the Carantinus can risk the lives of all of us

Periskopi (6 years ago)
(6 years ago)
Coronervirus ' disease, Covid-19, has been called the pandemic of the century. But it may, in fact, be the fraud of the century.) At the time that everyone needs the best information from the models of the disease and the governments to the people in quarantine, we all miss [...]
Coronervirus ' disease, Covid-19, has been called the pandemic of the century. But it can actually be the deception of the century. )
And at the time that everyone needs the best information from disease models and governments to people in quarantine, we all lack evidence about how many people are infected with SARS-CoV-2 or how many people are still getting infected. The best information is needed to lead to decisions and actions of monumentic importance and also to monitoring their impact.
Drakonic measures have been adopted in many countries. If the pandemic disappears on its own or because of these measures, we can somehow cope with social distance and quarantine. How long, however, will these measures continue if the pandemic does not disappear completely? How can policymakers tell us that they are not doing more harm than benefit?
Consistent vaccines and treatments take many months (or even years) to develop and test properly. In view of all the time required for them, the effects of long quarantine will be completely unknown.
The data gathered so far on how many people have been affected and how the epidemic is evolveing is quite unstable. Considering the limited testing so far, some deaths and perhaps most of the SARS-CoV-2 infections are not being counted. We don't know if we're failing to catch infections at the rate of error 3 or even 300. Three months after the blast, many countries, including the United States, have the majority of the ability to test large numbers of people, and no country has sustainable data on the spread of the virus with a common representational sample of the general population.
This evidence fissco creates great uncertainty about the danger of the dead from Coviddo-19shi. The reported mortality cases, like the official rate of 3.4 percent from the OBS, the horror sense of ? Patients who have been tested for SARS-CoV-2 are disproportionally those with severe symptoms and with great likelihood of infection. While most health systems have limited testing capacity, the prejudice over selection could get even worse in the near future.
A situation when an entire closed population was tested was the Diamond Princess yacht with its passengers in quarantine. The mortality rate there was 1,0%, but it was mainly due to the old population, for which the death rate by Ovid-19 is higher.
By designing the extent of the mortality at a non-compressive U.S. structure, it would be 0.0125%. But since these estimates are based on very little data because there were only seven dead among 700 passengers and the infected crew, the real death rate could range from five times less (0.025%) to five times more (0.625%). It is also possible that some of the infected passengers may die later, and that tourists may have a lot of chronic illness - a risk factor for bad results with SARS-CoV-2 infections - than the total population. Adding these sources to uncertainty, reasonable estimates of the mortality rate for the U.S. general population vary from 0.05 per cent to 1 per cent.
This huge change affects how serious the pandemic is and what we should do. The mortality rate of only 0.05% is lower than the seasonal flu. If that's the real scale, the world's closure and the terrible social and financial consequences of this thing can be totally irrational. It's like an elephant being attacked by a pet cat. Frustrated and trying to avoid the cat, the elephant accidentally jumps off the cliff and dies.
Could the mortality rate be this low by Ovid 19? No, some say, stressing the high degree of older ones. However, even some coronarys, called mild - tempered ones or the type of colds that have been known for decades, also had mortality as high as 8 percent when the elders infected.
These coronavirus “domestic” can be applied to thousands of deaths a year worldwide, although most of them are not documented by precise testing. They lost noise among 60 million deaths from various causes each year.
Although successful monitoring systems have existed for seasonal flu, the disease has been confirmed by a laboratory in a small number of cases. In the United States, for example, this season has so far tested 1 million and 73 thousand and 976 people for seasonal flu and 222 thousand and 552 of them (20.7%) had come up positive. In the same period, the estimated number of diseases such as the seasonal flu is between 36 million and 51 million, with a death toll of 22 thousand to 55 thousand.
Note the error march for deaths related to seasonal flu, corresponding to tens of thousands of sosh. Each year, some of these deaths are due to seasonal flu and other viruses, such as the soft “ ”.
In a series of autopsies tested for respiratory viruses in samples of 57 elderly people who died during the 2016 seasonal flu until 2017, flu viruses had been detected in 18 percent of samples, while species of respiratory viruses had been found in 47 percent of the cases. In some people who died of viral respiratory pathogens, more than one virus was found in their autopsy, and bacteria are often supermposed. A test for coronary does not necessarily imply that this virus is basically responsible for the patient's death.
If we assume that the mortality rate among the SARS-CoV-2 is 0.3% of the world's population and that 1% of the U.S. population is infected (about 3.3 million), this would be translated into 10,000 deaths. This number looks huge, but it's inside the palm tree. If we hadn't known about the new virus, and if we hadn't tested people with tests PCR, the number of total deaths due to “flu-like diseases” would seem unusual annually. At least, we would have noticed that the flu this season was slightly heavier than usual. Media coverage would be smaller than a NBA match.
Some worry that the number of 68 deaths from Coved-19 in the U.S. until March 16th will increase exponentially to 680, 66,000, 66,000, 66,000, 6000... just like similar catastrophic models around the world. Is this a real scenario or a bad ghost? When can we say that this curve will stop?
The most valuable piece of information to answer these questions would be to know the actual spread of infection to a common population sample and repeat this exercise at regular intervals of time to measure the incident of the new infection. Unfortunately, we don't have that information.
In lack of data, the reasoning “prepare-to-more-worse-worst” leads to extreme social distance and isolation. Unfortunately, we don't know if these measures work. Shutting down schools, for example, can reduce the rate of transmission of the disease. But they can fail if children become somewhat socialized if school closures cause children to spend more time with elderly family members if the children at home interrupt their parents ' work and so forth. Shutting down schools may lower the chances of demeaning immunity from the flock (hermunity) to a age group for protection from serious illness.
This has been the prospect behind the different position of Great Britain in keeping schools open, at least while I'm writing it. In this lack of data, we don't know if this perspective was brilliant or catastrophic.
The burden of cures to avoid overcrowding the health system is conceptually in order. A visualization that has become viral in the media and social media shows how the collapse of the cure reduces the volume of the epidemic above the threshold of what the health system can afford at any moment.
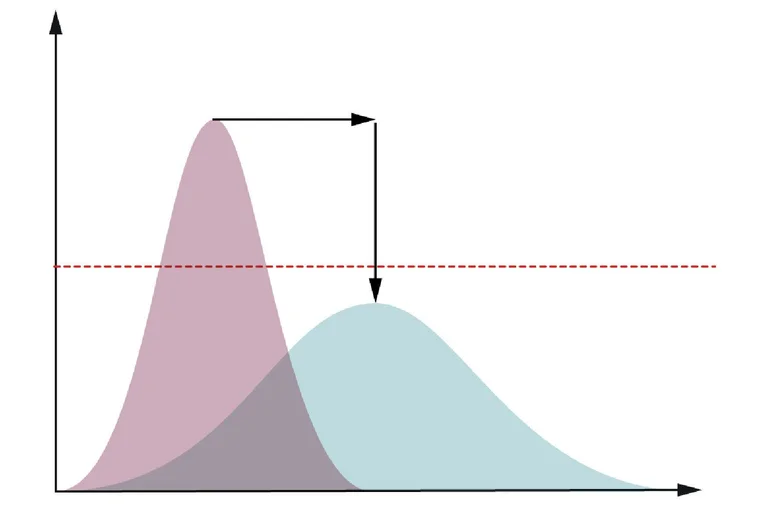
However, if the health system becomes impregnable by the coronary, most additional deaths may not be the cause of the coronary, but the cause of other diseases and other health conditionings such as heart attacks, trauma, bleeding, and others not treated properly. If the epidemic level invades the health system and extreme measures have only modest efficiency, this will only make it worse - rather than being conquered for an acute and short phase, the health system will remain occupied for a longer period. This is another reason why we need data for the exact level of epidemic activity.
And the big harm is that we don't know how long the social distance and quarantine measures will be maintained without causing major damage to the economy, society and mental health. Unpredictable developments may follow, including the financial crisis, uprisings, civil conflicts, wars and a social factory merger.
In the most pessimistic scenario, which I do not support if the new coronary infects 60 percent of the global population and 1 percent of the infected die, this will translate into more than 40 million deaths globally, as much as the Spanish flu pandemic in 1918.
The vast majority of this slaughter would cling to people who were expected to die within a short period of time, which is the contrast of 1918, when most of the dead were young.
We can only hope that, as in 1918, life will continue. With quarantines lasting for months, if not for years, life will be stopped, and short and long-term consequences are completely unknown, billions, and not just millions, lives endangered.
If we decide to jump off the rock (such as the elephant because of the cat), we need more data to inform us of the reasonableness of these actions and chances of falling somewhere we can save somehow.
John P.A. Ioannidis is professor of medicine, epistemology and population health, biomedical data science, and statistics at Stanford University, and co-director of the Stanford Center for Meta-Research Innovation.
This article is translated into Albanian by Periscope. We send out other newspapers that are interested in copying it on their pages to quote our newspaper.