Pilonal sin, or guitar, filled with the presence of deep - seated hairs

Periskopi (3 years ago)
(3 years ago)
There are some more complicated technical terms related to this situation, such as the pelonal guitar or the sacrocococgeal tribe, but in fact it is widely known under the term “continent”. This situation represents the formation of a key or limited purulent inflammation (absces/cells) located in the glucose fold. Only one cyst may appear in some patients, [...]
This situation represents the formation of a key or limited purulent inflammation (absces/cells) located in the glucose fold. In some patients, only one cyst may appear, while some may develop a tribal trajectory. In most cases, the surface of the skin provides an opening through which the purulent content is derived.
This situation was described for the first time by Hodges in 1880, and a few years later Herbert Mayo described the same situation as a <x0-kiss filled with”
This problem is typical of men. A higher frequency of this problem has been observed in soldiers. In World War II, it has also often been observed in the drivers of four - wheel - drive vehicles and heavy combat vehicles, so this condition was also called a Diesian jeep disease.
Epidemiology
The infection of this disease is considered to be 26:10,000 people. In the last 50 years, there has been an increase in the number of affecteds, for which greater use of motor vehicles and computer use has been recorded. Such a way of life leads to a sedentary (slown) way of life for the entire population.
As for spreading this problem, the disease is more present in men than in females, and the ratio is 4:1.
Besides the reason I have to do with lifestyles, the incisor is higher in men because of greater perspiration and presence of hair in the interglute area. As to age, this disease usually appears in people in the second and third decades of life.
Ethiology
The exact reason that leads to the appearance of the pilonal synous is still unknown, yet there are several theories that explain its appearance. Theories are divided mainly into two types: the result of genetic factors and the theory of showing under the influence of risk factors.
The theory of genetic predisposition indicates that pilonal sinus is an inborn skin abnormality in the upper part of the buttocks, which may occur because of an embryoic residue of primitive notords in the skin of the area. Later in life, this affects the gathering of dead skin cells and skin fibers, which then produces an inflammatory process that follows the formation of a purulent collection.
The theory showing the pilonal synnus under the influence of risk factors involves:
- Overwhelming in the glucose area
- Overweight ʹ obesity
- The Family Trend
- Male Persistence
- Profession related to prolonged decline
- Deep Break or Hurt in Interglutal Zone
- The presence of multiple hairs
- Poor Hygiene in the Body
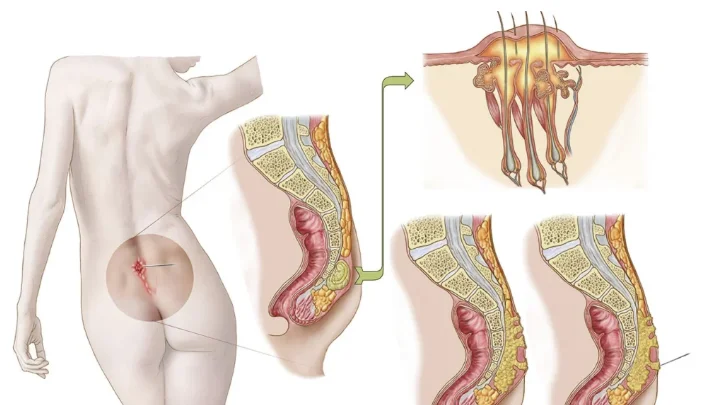
Clinical view of the pilonal sinus
In one part of the patients, the clinical view of the pilonal synus may be without any signs or symptoms. While there are those who experience skin changes in this area. These resulting changes can be very painful, followed by an inflammatory process of skin in the form of an underwater key that breaks into the next period and spills the purulent (sored) or bloody content.
Because of the pain in the area shown, patients complain of falling difficulties and unable to walk. After the corrupting of the guitar and its content, there is relief, but it is short - term because after a certain period of time, the collection of purulent content within the cast.
Although the pilonal sinus is more characteristic for its appearance in the mushroom (cross) area, its performance is also described in:
- Spacing between fingers
- The armpit area
- About the umbilical belly button
- In the intermarare area (mixing bays)
- The genital Zone in both males and females
- Amputation waste (in the amputation area)
Diagnosis
The diagnosis of the pelonal synnus is established on the basis of the patient's anatomy and clinical examination. In certain cases, a diagnostic method that shows the subterranean extent of change itself can be carried out. During the diagnosis, since the skin in the mushroom area is in close contact with the rectum, a digital anal manual examination may be required.
Preparation Before the Operation
In agreement with the surgeon, both for any other operation and during the operational treatment of the pilonal synus, pre-activation is required. This preparation involves:
- If it has purulent content, it is mandatory to take a tampon (bris) for microbiological and antibiogram analysis at least 7 days before planned operating treatment.
- Empty the gastroinstinal leftovers with the help of the lactators.
- Standard pre-activial preparation for surgery under general anesthesia.
The surgical treatment of the pilonal sinus
The surgical treatment of adult under the skin can be performed under local anesthesia. But for greater comfort to the patient, surgery under general anesthesia is recommended. After the operating field toilet (cleanage) injection requires an injection of the blue methyle in the tribal channels. If the solution to the blue methyle is not available, injections with iod personone may be administered. This procedure is aimed at painting/ignoring the modified tissue (literated) in order to be marked/distinguished by healthy tissue.
Once the gap is made, the surgical removal of the altered tissue is made to the achievement of healthy macroscopic tissue (obvious to the eye). Thus, the remaining tissue of the changed tissue is avoided, avoiding repetition of the pilonal sinus. The altered tissue that has been removed must be examined by a pathologist to establish a final pathofiastic diagnosis.

Postoperative Treatment
After surgery, patients remain in hospital for at least one day. Depending on the clinical appearance and condition of the posttoperative wound, the patient may need to continue treatment for several days. Usually, after surgery, the patient stays in the hospital for another two days.
In the postoperative period, to prevent mechanical damage from the surgical sewing, the patient must lie in the womb for the first 48 hours. On the first day after surgery, avoid taking food to avoid the need for emptying, which could lead to a show of potential complications. The patient is advised that during the day, after conducting the operation itself, to avoid movement/takeoff and to strictly stop sitting with open legs (relaxed in a relaxed manner). On the first day after the operation, there is a victim of the wound to assess its posttoperative state.
In the following period, after being released from the hospital, the surgeon gives instructions for further home treatment on surgical treatment as well as sanitation and dietary advice. After the surgery of the pilonal synnus, the patient is willing to return to work three weeks after surgery and after a mandatory examination by the surgeon himself who has conducted the intervention.
The Most Often Questions
Is there a risk of cancer in the changed tissue?
As for clinical appearance and clinical characteristics themselves, one of the differential diagnosiss of the pilonal synnus is scynomous carcinoma. To establish an exact diagnosis, it requires an examination by a specialist who can distinguish between the pilonal synnus and scnomenous cell carcinoma based on clinical examination.
Is there a danger of repeating the pilonal synus after surgery?
Of course, there is the possibility of repetition, so during operating treatment, there is a distinction of tissue in which the tissue limit altered by healthy tissue can be determined.
Is it possible to treat pilonal sinus without surgical treatment?
If it's an initial change that hasn't shown underground channels (Ustula) and is limited, without the presence of public or bloody secretation, changing lifestyles, that is. Changing dietary and hygienic habits, it is possible to heal without surgery. But in each case, examination is required by a plastic surgeon.












