Interview Dr. Ambbarkova speaks of deep veins: Here's what you need to know

Periskopi (3 years ago)
(3 years ago)
Deep veins are a serious disease that often has no symptoms and therefore is revealed very late - a fact that can lead to pulmonary embole, which can be fatal. How do deep veins clots appear, and why does it occur? The venous trombobolism is a serious illness that represents a [...]
Deep veins are a serious disease that often has no symptoms and therefore is revealed very late - a fact that can lead to pulmonary embole, which can be fatal. How do deep veins clots appear, and why does it occur?
Vesssinous Trombbolism is a serious illness that presents a major health problem and is one of the most frequent causes of hospital mortality, which can hopefully be prevented.
“Vermombalism manifests itself as deep ventrosis and pulmonary emboli. Deep veins are a condition in which a trumpet is created in one of the deep veins, most frequently standing but is not disfellowshipped to appear in the veins of the hands or organs assigned to the body. Elena Ambarkova Willarova.
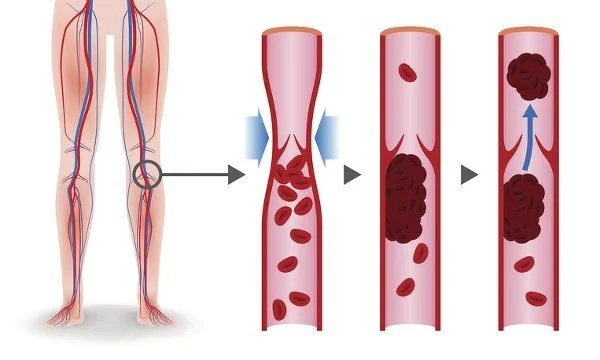
For the formation of the trumpet in a deep vein, three conditions must be met at the same time: slowdown of the leak through the vein, increased blood clotting (hyperhagulation) and damage to the caterpillar wall. If the trumpet formed in the deep vein is released, it travels through blood vessels to one of the arteries in the patient's lungs, blocking the flow of blood into the lungs, a condition called pulmonary emboli.
Overweight, tobacco consumption, standing or sitting for a long time... What other risk factors contribute to the development of deep veins?
Three conditions, or risk factors, for showing the trumpet in the vein are met by certain conditions. Increasing the tendency to form blood clotting is otherwise known as thromorphilia. Some of the factors leading up to the trombophilia are born or inherited, in such cases we cannot influence them, and they usually lead to the trumpet's appearance in the deep veins of younger veins (under 50 years), but some strokes are acquired during life, and in this case, the concentration of preventing the disease.

Born or inherited factors that contribute to a significant increase in risk of developing this disease are the V Leiden factor and the mutation in protrombin. A Lack of Antitrombin III, the protein C and S may be congenital and acquired, and the appearance of anticoagulants of lupus and antiphosfolipide antibodies can be associated with other diseases. The most common factors acquired to increase the risk of showing the trumpet in the veins and in which, after due evaluation, the exposure of this disease can be prevented by using preventative doses of anticoagulant therapy:
• Long emotionalizations during hospital stay or paralyzed patients
• Trauma, orthopedic surgery of the lower limbs
• Myocard patients, stroke, spinal cord damage
• Previous trombosis of deep veins (due to damage to the vein wall), variable veins
• Other hematological diseases (e.g. lettuce, kidney disease (the nephrotic syndrome), bowel disease (lacterosis), autoimmune disease, mountain disease.
• Medical therapy (ortal contraceptive transplants, other substitute hormone therapies, anesthetics)
• The venerous trauma ítra venosis central, usually located in the upper extreme.
• Age increases the risk of thrombosis, and unfortunately it is one of the factors we cannot control.
What effect does pregnancy have on the growth of this situation, are pregnant women exposed to a greater danger, and what should be taken care of?
• The pregnancy is a physical, hypercogmatic state. During this period, certain clotting factors increase, and natural anticoagulant activity decreases because the mother's body prepares for the act of birth in order to prevent post - birth bloodshed. Vennosis is not a normal pregnancy state, but it can occur at any time during pregnancy and six weeks after birth. Rarely, deep veins may occur until the third month after birth.
• The operational birth (Cesarean birth), the complications during pregnancy or after birth, chronic diseases in pregnant women, such as heart disease, lung disease, or diabetes, are also risk factors in showing deep venosis.
• The presence of genetic factors for thromorphilia, as well as the presence of antiphosphoptide antibodies to the pregnant woman, leads to an increase in the physical hypercognosis of blood, and may result in other complications in pregnant and fetus, for example, repeated spontaneous abortions, delayed fetus growth, late abortions, dead births, and preeclampsia. Managing women with high blood clots of high blood pressure, visible ventricle tombosis, or stroke - related complications is complex and requires a multidisciplinary approach, including gynaecologist-obberian doctor, a transfusion doctor, and other specialties doctors, depending on the chronic illness that a pregnant woman has.
Acute tyres of deep veins up to 50% of the time do not have specific symptoms, but when they are present, what are the most common signs showing that this situation is present?
Unfortunately, the patient may very often have no symptoms or just a discrete swelling or undefined pain in the skin or thigh. When dealing with a more serious situation, the first symptoms may appear as pulmonary thrombosis with chest pain, breathing difficulties, blood explosives. pulmonary or lung embolia is a potentially life - threatening state and requires immediate treatment and, in more serious cases, compulsory hospitalization.
Symptoms of deep veins in the most common area are:
• Pain and/or cramp on one leg (skin on both legs), usually on the belly of the foot
• The ring of one leg (foot on both legs)
• Skin heat
• Red or dark skin
• Visible superficial veins may appear.
• The same symptoms appear during the trombones of deep veins in hand or in other areas.
How is diagnosis established?
Medical Test D-Dimer If this test is negative (in terms of reference limits), then with high probability it can be expelled from ventrosis. If the test is off limits of reference and we have a clinically high suspicion of YEARS, then, we need to go a step further with diagnostic methods (designed below) to confirm or exclude the presence of the VTE. This test is also positive for other conditions (inflammatory processes, normal pregnancies, malaria, heart attacks, and other diseases).
Ultrasonography ) Doppler Ecography of deep and superficial veins is a noninvasive method in which a doctor easily passes the skin of limbs with the help of the probe, following the course of the vent. By doing so, the screen visualizes changes in blood veins, their functionality, and the presence of blood clotting in deep, superficial veins.
Flebography An angiographic invasive method for visualizing the vnosis system in contrast. Although earlier this method was <x0ndandraded gold” in the diagnosis of deep veins, it is now replaced by ultrasound as a noninvasive method.
Computerized pulmonary Angoography ) “
Ventim ) scan for fusion A method of detecting pulmonary embolia using radioactive substances. It's used less often to patients with counterindication for pulmonary computer angiography. The same is true of pulmonary agiography, which is an invasive diagnostic method.
Magnetic Rezonion This is not the first method of diagnosis of the VTE and is used by patients to whom radiation has been counterindicted (e.g. Pregnant women).
What is the treatment of the deep veins (VTE) to which?
The treatment of the VE is done with anticoagulants. Their “hone” blood and prevent trumpet growth. These include heparina, vitamin Entagonists K, or drugs taken in a specific pattern that is appropriate for each patient and is rendered against value INR that is determined through a patient's blood test.
vitamin antagonists K (acenocumarol,warfarin...) have a variable anticoagulant effect that depends greatly on the way of life, especially on diets and other medications that the patient receives. In the last ten years, new anticoagulant drugs (rivaroxaban, dabigatran, apixaban...), which patients can receive without regular blood tests, and at the same time matter little to diet and other drugs.

Anticoagulant therapy is usually given in 3-6 months, but high - risk VTE patients can be given throughout life.
Fibrinotic drugs (trains that make up “include <x1m> thrombin) are rarely used in the treatment of venosis clots because of increased risk of bleeding complications. These drugs, as well as surgical methods for the removal of the trumpet, are used in extraordinary life - threatening conditions as a result of the VTE.
Compression therapy, so flexible socks, usually with compression class 2, is recommended that in the first month following the appearance of deep-foot veins, to prevent post-trombotic syndrome. Post-trombotic syndrome is manifested by a series of symptoms such as the sense of gravity in the leg, the scratching, the swelling, the worsening pain of standing, the enlarged veins (varics), the change of skin color, and the display of ulcers (lags), symptoms that may largely damage the quality of the patient's life.
What are the precautions that each of us can take to reduce the risk of deep veins clots? When are compression socks recommended?
General recommendations for all of us regarding the prevention of the VTE are the same as for all cardiovascular diseases, physical activity, and the preservation of optimial body weight, balanced diet, smoking, good hydration.
A particular category of VTE prevention are patients who have already had a VTE episode or have a close family member with VTE history or have risk factors that increase risk for YEARs we've already discussed.
In our hospital, all patients who have been laid down for a health problem or surgical surgery are assessed for the risk of the VTE for accession, and are properly protected by the historical dose of anticoagulant therapy.
For such patients, there are also special recommendations on frequent and long trips by plane, car, bus, or train. The same recommendations must be practiced by all passengers, so some airline companies have prepared protocols they display on the monitor during long - distance flights.
• Moving as Long as You Travel
• Wear pre-emptive anti-embolic socks
• Muscle exercise at the lower knee
• Avoid alcohol or soothing (which may limit physical activity)
• Good hydration
• Seek immediate medical care if there is swelling, chest pain, or breathing difficulties
• In some cases of extremely high risk of FTE, the doctor may also recommend preventative doses of anticoagulant therapy.












